
Case Report
THORACIC DISC PROTRUSION/EXTRUSION AT T10/11 TREATED WITH COX® FLEXION-DISTRACTION THERAPY: AN ONGOING ANALYSIS.
AUTHORS: Dr Danica Newbold (B. HSci (Chiro), M. ClinChiro, Ad. Dip. Myotherapy, Certified Cox® Flexion-Distraction Practitioner) & Dr Joel Dixon (B. App.Sc (Chiro), J.P., Certified Cox® Flexion-Distraction Instructor); Malvern Chiropractic & Melbourne Spine Clinics (Melbourne, Australia)
CLINICAL HISTORY
Mr P presented to Malvern Chiropractic Clinic and Melbourne Spine Clinic (Melbourne, Australia) on 30th November 2021. He indicated five (5) years of mid to lower thoracic pain radiating around the left lower costal margin and into the abdomen. He associated this pain with a series of manual handling incidences whilst working at his farm. At the time of the incident, he experienced excruciating neck and thoracic pain, which eventually subsided. Recently, he described the thoracic pain as a “burning sensation” and rated it as a 5/10 (VAS Score).
Mr P explained that his pain worsens when driving in the car and leaning over at work (i.e., over a bench) and is relieved by walking and standing upright. Mr P noted that his pain affects his sleep quality and quantity, and decreases his energy levels and concentration. It also interfered with his work and activities of daily living (ADLs).
Previous management included Physiotherapy treatments, over-the-counter (OTC) analgesics, and anti-inflammatories
Mr P had an MRI study performed in the first half of 2017 following previous manual handling farming incidences, which included long hours of fencing, i.e., heavy lifting and repetitive bending and twisting. The report was presented and reviewed at the initial consultation in our clinic.
EXAMINATION
An initial examination performed on 30th November 2021 revealed the following:
Range of Motion (ROM): Thoracolumbar ROM (active) was mildly reduced in all planes, most notably in left lateral flexion and rotation, with mild pain at the end range.
Palpation: Hypertonicity and tenderness was noted at the lower thoracic Erector Spinae (ES) muscles (L>R), Quadratus Lumborum (QL) (L>R) and the thoracolumbar portion of the Latissimus Dorsi (L>R). Spinal joint tenderness and rigidity were noted over the T8-T10 spinal levels bilaterally.
Neurological and Orthopedics: Lower limb reflexes we tested were within normal limits.
Myotomal screening revealed mild weakness in the thoracic extensor muscles with mild pain reproduction and resisted lateral trunk flexion (L>R).
Orthopaedic testing returned positive results for:
- Slump test – localised pain around the T8-10 region
- Supine Straight Leg Raise (SSLR) – No leg pain; however, localised pulling sensation was noted at the thoracolumbar region (L>R).
- Schepelmann’s Test (arms fully abducted above head, the patient is instructed to flex torso left and right laterally. Positive indications for nerve root impingement) – the patient noted pain on the left T8-10 region with very mild pain in the left lower costal region.
- Soto Hall – very mild localised pain around the T8-10 region (L>R).
IMAGING
Mr P underwent an MRI study of his abdomen and thoracic spine on 11th April 2017. The report for this study was presented at the initial consultation. The radiologist reported the following:
- Central to right paracentral disc protrusion at T10/11, which demonstrated a small cranially directed extrusion component indenting the right anterior hemicord resulting in mild central canal stenosis.
After commencing care in our clinic, Mr P noticed slight changes in his pain and its referral to the abdomen; however, in early February 2022, Mr P experienced a flare-up of his condition. Repeat MRI studies were referred by our clinic and performed on 9th March 2022. The radiologist reported the following:
- Large right paracentral T10/11-disc extrusion compressing the right ventral spinal cord measuring 12mm mediolaterally, 7mm anteroposteriorly and 9mm superoinferorly.
- At T7/8, there is a very mild posterior disc protrusion causing mild thecal sac indentation.
- T8/9 is a mild right paracentral disc protrusion with annular fissure causing mild right ventral cord indentation.
Given the metrics established in the second MRI scan, we asked Mr P if he had the original scan images. We received a CD of the images and requested a comparative interpretive assessment of the two MRI scans. Based on the addendum added to Mr P’s March 2022 MRI report, the radiologist measured the original scans of the previous disc lesion as 9mm mediolaterally, 6mm anteroposteriorly, and 11mm superoinferiorly. See the table below for the side-by-side comparison (Fig 1) of the T10/11-disc protrusion/extrusion metrics.
| MRI 2017 | MRI 2022 | Difference | |
| M-L | 9mm | 12mm | + 3mm |
| A-P | 6mm | 7mm | + 1mm |
| S-I | 11mm | 9mm | – 2mm |
Fig 1: Comparative analysis of the T10/11-disc lesion.
Please refer to the images below of the initial 2017 MRI scans and the most current 2022 scans (Fig 2a,b and Fig 3a,b).

Fig 2a: Thoracic Spine T2 Mid Sagittal (11/04/2017)
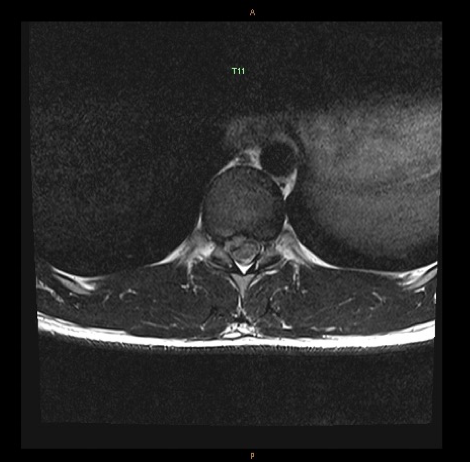
Fig 2b: T10/11 Disc T2 Axial (11/04/2017)

Fig 3a: Thoracic Spine T2 Mid Sagittal (09/03/2022)
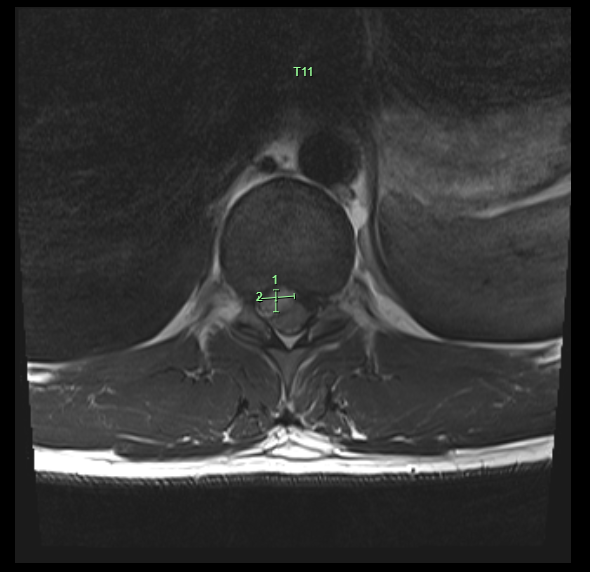
Fig 3b: T10/11 Disc T2 Axial (09/03/2022)
TREATMENT AND RESULTS
Mr P has been receiving Cox® Flexion-Distraction and Spinal Decompression Therapy since his initial presentation, focusing on the T10/11 discal protrusion/ extrusion. Whilst Mr P maintains that his pain is consistently left-sided despite the imaging indicating right-sided involvement, his treatment plan has focused on the patient’s signs and symptoms.
At session one (1), the patient was informed about all aspects of the Cox® Technic, and treatment began. Following tolerance testing, Flexion-Distraction Protocol I (1) was applied to the thoracic spine above the left-sided T8-T10 discal compartments (“5-4-3 Method” – 5 repetitions, over 4 seconds in groups of 3) and soft tissue therapies using an electric percussion therapy tool to the thoracolumbar region. The patient was advised to conduct self-care at home post-treatment consisting of rest and cryotherapy (cold/ice packs) – 10 minutes of cold/ice pack applied 3 to 4 times over 24-48 hours post-treatment.
Mr P had a follow-up appointment two (2) days later on 2nd December 2021, with no increased pain or discomfort but no change in VAS since the initial presentation. Protocol II (2) Flexion-Distraction Therapy (long y-axis traction, flexion, lateral flexion by ten repetitions at approximately 50% intensity) was performed to the same thoracic levels (contact above the left T8-10) with good tolerance. Treatment included targeted soft tissue therapies to the thoracolumbar regions.
By session four (4) on 13th December 2021, Mr P’s VAS score had decreased to 2/10 (50% improvement). Flexion-Distraction Protocol II (2) therapy continued to full intensity with the same focus on the levels above the left-sided T8-10 discal compartments. Mr P was advised on adjusting and maintaining appropriate posture and ergonomics whilst at work as this seemed to be the more stressful element for his spinal pain. We introduced regular breaks from bending/ leaning over every hour and advised, where possible, to slightly increase the height of his work area so that he could avoid bending/leaning over too far.
At session five (5) on 20th December 2021, Mr P continued to show signs of improvement. His pain levels were still milder than the initial presentation, the referral pain into the left lower costal margin and abdomen had decreased in intensity and frequency, and he still described a stiffness in his thoracic region. Flexion-Distraction Protocol II (2) was still the primary treatment utilised to treat Mr P and targeted soft tissue therapies. He was prescribed spinal stretch exercises using an inflatable exercise/gym ball to reinforce the decompressive force of the treatment being applied to the discal compartments.
With the holiday period approaching, there was a small gap in the treatment frequency, and we were able to pick up again just before the New Year’s Holiday break. The pain had slightly elevated with the increased activities associated with Christmas celebrations but settled with rest and the previously prescribed stretches. After New Year’s, the pain was more intermittent, and he noted that he experienced “a couple of days of relief here and there”. After returning to work post-holidays, Mr P stated that his thoracic tightened up whilst working; however, he was getting more relief overall.
In early February 2022, Mr P had re-aggravated his thoracic spinal pain, resorting to the original pain levels, signs and symptoms. Mr P associated this with an increased workload and repetitive bending and manual handling whilst fencing on his farm. At this time, we gave Mr P a referral for new imaging to investigate the cause of the increased pain he was experiencing.
PROGNOSIS
Mr P’s progress through the treatment program has been tempered; He has shown moderate improvement in his pain levels and ranges of motion. He continues to work in a highly manual handling role as a diesel mechanic, which has meant repetitive irritation and aggravation of his spinal disc pain. He has found some comfort in his daily life. He is more energetic and can get more rest/sleep. Mr P is also able to get back to complete some of his normal activities of daily living (ADLs). However, he is continually re-injuring his vulnerable spinal disc due to his work environment and never truly finds complete relief in his pain and symptoms.
Re-evaluation of the initial MRI scans revealed an increase in the mediolateral and anteroposterior projections of the T10/11-disc protrusion/ extrusion (M-L +3mm, A-P +1mm) when compared to the latest scans and report. Further deterioration noted in the newest report indicates early signs of disc disease and protrusions at the T7/8 and T8/9 levels. There has been some retraction of the superoinferior projection of the T10/11-disc protrusion/extrusion (S-I -2mm).
A re-examination of the patient’s original signs and symptoms demonstrated that the thoracolumbar Range of Motion (ROM) was slightly reduced in all planes but was more symmetrical than the initial examination. Orthopedic and neurological tests revealed similar findings to the initial assessment; however, any pain reproductions were slightly milder in intensity. Palpatory findings still demonstrated mild hypertonicity and tenderness of the long spinal muscles in the thoracolumbar spine and tenderness and rigidity of the T8-T10 zygapophyseal joints (L>R).
Mr P continues to receive Chiropractic spinal disc decompression using Cox® Flexion-Distraction Technic on a weekly basis. He still notes intermittent pain with spinal stiffness associated with work and, on occasion, some milder referral pain into the left costal/ abdominal region. We have sought a surgical opinion and have compared the conservative versus surgical outcomes. With more significant improvement in Mr P’s condition, Mr P will progress through the treatment program and eventually to a long-term maintenance style plan that will continue to monitor his spinal joint mobility and disc degradation and introduce further exercises and rehabilitation to stabilise his condition.
CONCLUSION
Mr P still demonstrates mild symptoms consistent with his initial presentation. This is also shown by the latest MRI scans that Mr P underwent. The latest report states that the thoracic disc protrusion/extrusion at T10/11 has decreased in the superoinferior aspect and increased at the mediolateral and anteroposterior projections. This may result from repetitive wear and injury to the discal compartments as a consequence of the manual handling roles he performs regularly. The retraction of the superoinferior direction of the T10/11-disc protrusion/extrusion is a positive outcome for Mr P’s condition. It may explain why he initially noticed a slight decrease in his pain levels and symptoms with the application of Cox® Flexion-Distraction Therapy.
Cox® Flexion-Distraction and Spinal Decompression therapy has allowed this patient some relief in his overall signs and symptoms and therefore has been the appropriate treatment method for this patient’s condition. With continued therapy and modifications to the patient’s workplace activities, we believe that Mr P should find further reduction in the thoracic disc protrusion/ extrusion and, therefore, in his pain and mobility. Constant communication and examination with the patient are crucial to establishing future outcomes and hopefully resolving this condition.
REFERENCES:
- Cox JM, Feller J, Cox J. Distraction Chiropractic Adjusting: Clinical Application and Outcomes of 1000 cases. (1996).
- Gudavalli MR: Estimation of dimensional changes in the lumbar intervertebral foramen of lumbar spine during flexion distraction procedure. Proceedings of the 1994 International Conference on Spinal Manipulation, June 10‐ 11, 1994, Palm Springs, CA, pp 81.
- Gudavalli MR, Cox JM, Baker JA, Cramer GD, Patwardhan AG: Intervertebral Disc Pressure Changes During a Chiropractic Procedure. Proceedings of Bioengineering Conference, Phoenix, 1997