
Case Report
Changes in a Lumbar Disc Extrusion After Cox Technic Flexion Distraction Therapy in a 44 year old Office Worker
Submitted by
Dr Joel Dixon B.App.Sc (Chiropractic) J.P. Melbourne Spine Clinic Melbourne, Australia
Dr Chloe Wilkinson BBiomedSc, BHsc(Chiro), MClinChiro (Dist) Malvern Chiropractic Clinic Melbourne, Australia
HISTORY
Mr JD
DOB: 24.03.71
The patient is a 44 year old male who presented to the Malvern Chiropractic Clinic on April 2nd, 2015 with right-sided low back pain radiating into the posterior thigh, leg and foot, with numbness distributed over the same pattern.
The pain started three weeks prior on March 11, 2015; he was admitted to the Alfred Hospital, Melbourne, Australia, for pain management and was discharged the same day. His condition had been described as a disc bulge with sciatic radiation.
The patient described the pain intensity as a 3/10 VAS scale with a stable nature, aggravated with tennis, when getting out of his vehicle and lifting and only relieved by lying in a supine position. He reported that the pain was interfering with his normal daily routine including sleep, work and exercise.
There is a previous history of low back pain 20 years prior following a football injury, believed to be the same spinal vertebral level, with previous treatment administered by an osteopath and physiotherapist.
His last therapy prior to consultation was by a physiotherapist 3 weeks prior. The patient had consulted with a neurosurgeon who had recommended microdiscecomy at L5/S1 level.
Physical Examination:
Palpation:
Bilateral spinal muscle contracture from levels L3 to S1 with right leg, posterior thigh, posterior calf and foot pain.
Range of Motion:
Active and passive lumbo-sacral range of motion was diminished by up to 50% in all 3 planes of movement.
Orthopaedic examination:
Seated straight leg raise- right side positive at 60 degrees and 70 degrees on the left.
Kemps test was positive on the right side and a functional short leg was positive on the right side by up to 20mm.
Neurological examination:
L4 deep tendon reflex- right +1, left +2 L5 deep tendon reflex- right 0, left +1
Myotomes- Extensor hallucis longus (EHL) right side weakness compared with left side
Dermatomes- right side dermatomal distribution demonstrates paraesthesia and anaesthesia patterns
Imaging:
Three lumbo-sacral spine MRI’s were conducted on the 30th March 2015, 6 weeks later on 14th May 2015 and 5 months later on the 25th November 2015.
The initial films revealed a very large disc extrusion of L5/S1, lying posterior to the S1 nerve at disc level, compressing it anteriorly against the disc. There is a large volume of abnormal tissue following the S1 nerve down into the S1/2 lateral recess. Figure 1
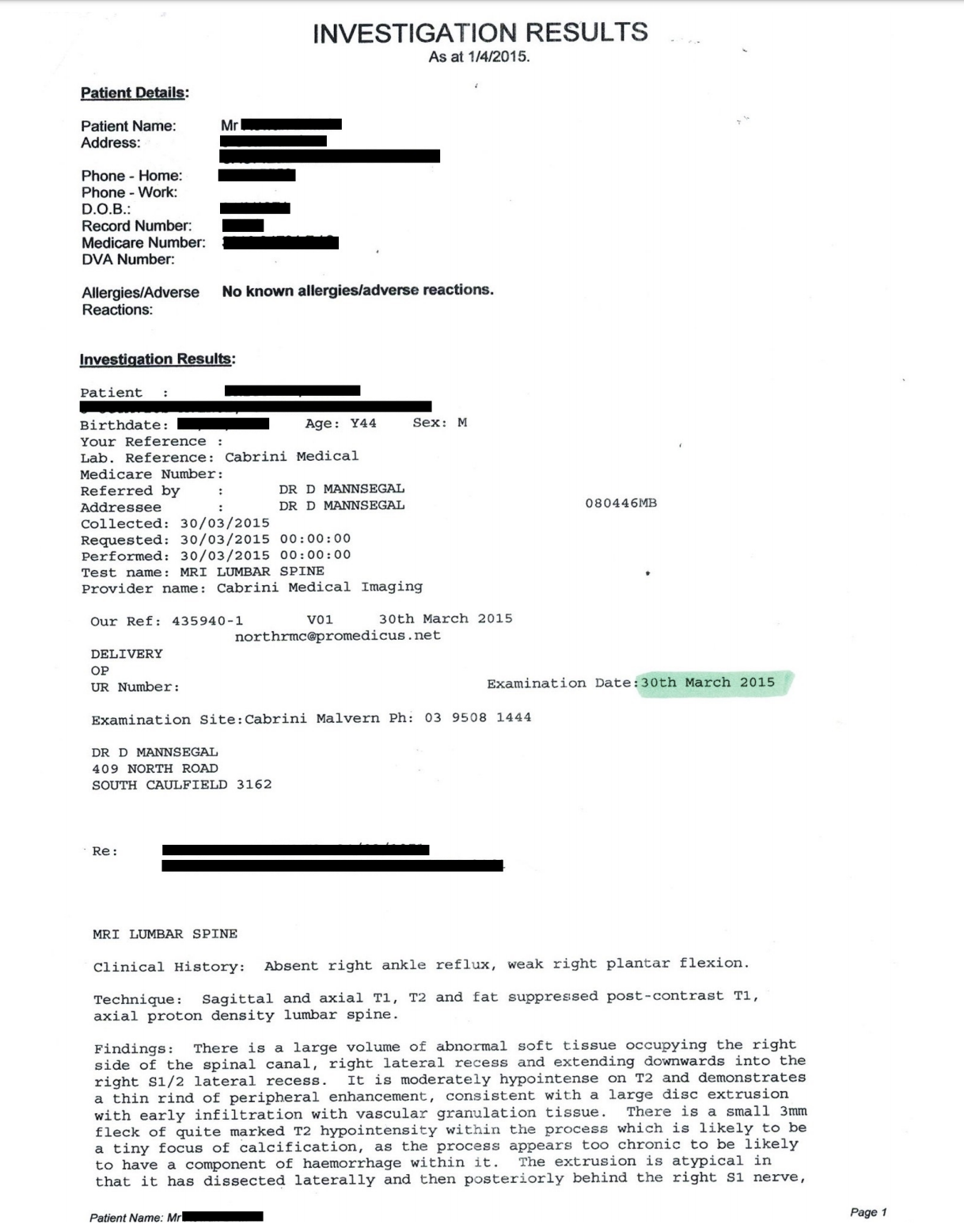
fig1.1
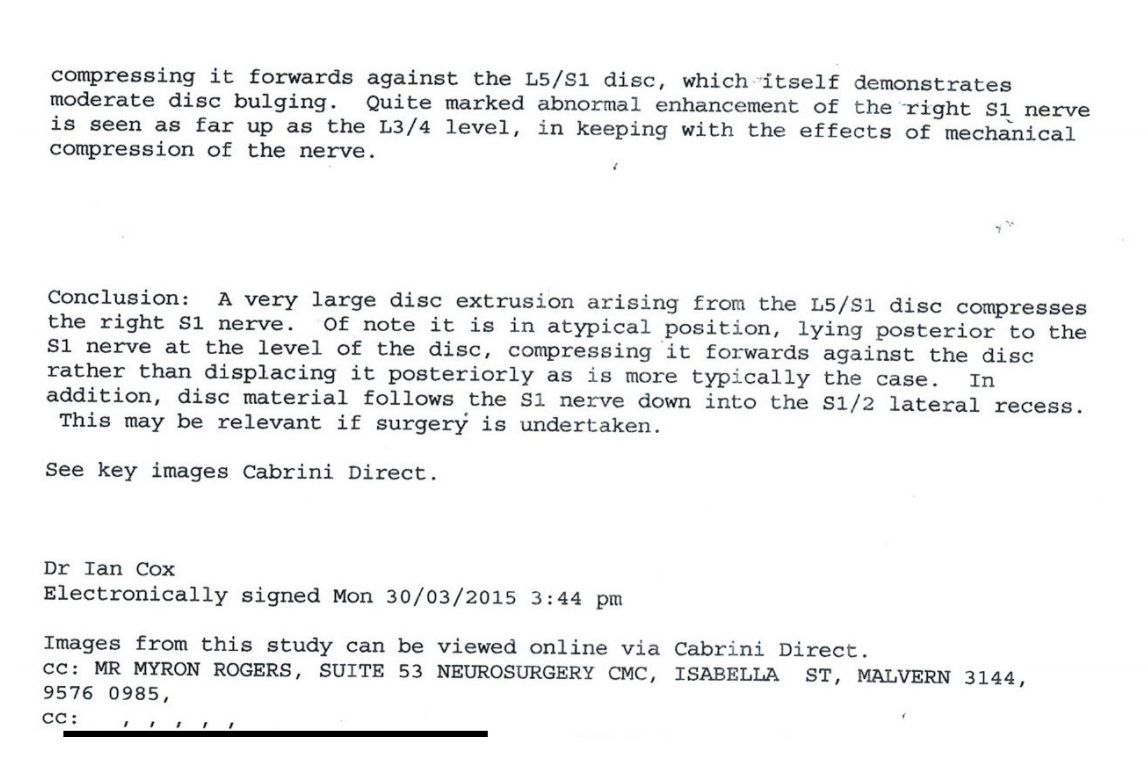
fig1.2
The following MRI taken 6 weeks later on May 14th, 2015, found a moderately reduced disc height of L5-S1 disc with discophyte anteriorly and a spur in the right L5 foramen not contacting the L5 nerve. This was much improved in comparison with previous imaging. Figure 2
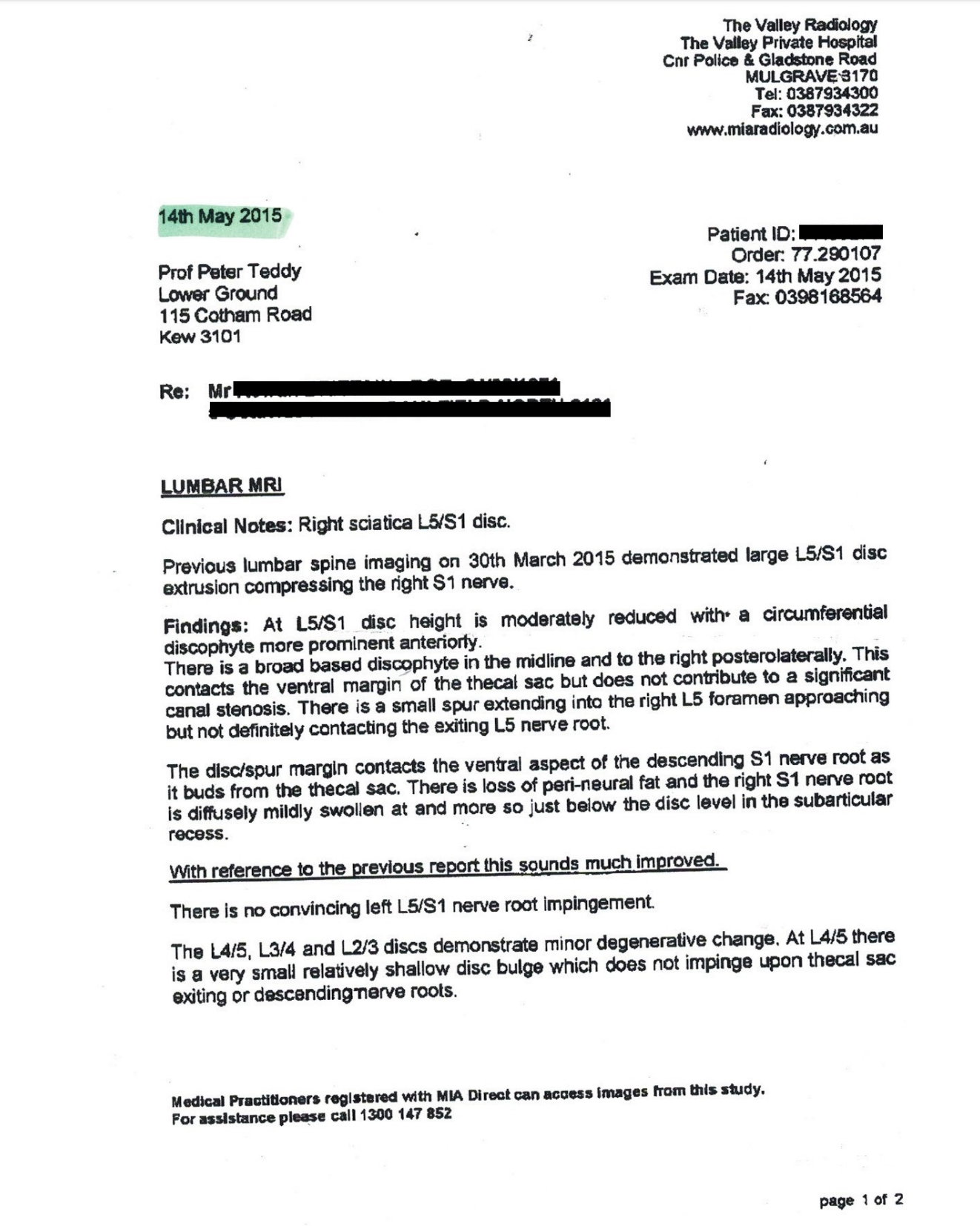
Figure 2
The most recent MRI conducted on November 25th, 2015 showed a mild broad based L5/S1 disc bulge with right postero-lateral annular fissure. There was mild contact and displacement of the right S1 nerve. Scarring and thickening around the right S1 nerve had decreased since previous imaging. Degenerative end plate change and desiccated L5/S1 disc were evident. Figure 3.

Figure 3
Treatment:
The patient was treated with Cox Technic flexion- distraction spinal decompression therapy protocol 1 consisting of long axis/y axis distraction and protocol 2 including circumduction motions (5×4 decompression sets), both focusing on the right sided discal compartment. Soft tissue therapy and a prescription of core stabilizing exercise and stretching routine were also administered.
The initial course of care was twice weekly for 5 weeks, once weekly for a following 4 weeks and once fortnightly between April 2015 and January 2016, with 40 treatments in total, maintaining an 80- 100% reduction in pain.
Cox flexion distraction, disc decompression therapy has been demonstrated to both diminish the size and pain impact of the discal pathology and its further impact on the compromised DRG.
Prognosis:
Patient progress has been excellent and he is expected to return to all normal ADL’s including non ballistic recreational activity.
It was explained to him that long term success was a result of a balance between an active and passive mobility programme and hence he has been given appropriate stretching and core strengthening routines .
We have also assessed and modified workplace and domestic ergonomics.
I am confident that self management along with supportive Cox Decompression therapy will maintain this patient’s low back condition well and help him get on with pain free ADL’s.
Conclusion:
The appropriate application of Cox flexion-distraction therapy protocols in this case has:
The appropriate application of Cox flexion-distraction therapy protocols in this case has:
1. Significantly reduced both signs and symptoms associated with discal compartment pathology and the associated Dorsal root ganglion compression consequences.
2. Resulted in the MRI changes demonstrated over three separate images over a period of some 7 months.
3. Significantly reduced intradiscal pressures at L5-S1 level and a tightening of the posterior longitudinal ligament (Gudavalli et al 1998) may explain the reduction in discal mass extrusion postero laterally into spinal recesses at this level.
References:
1 ‐ Cox JM: Low Back Pain: Mechanism, Diagnosis, Treatment, 6th edition, Baltimore; Lippincott Williams &Wilkins, 1990, Chapter 8, Appendix B.
2 ‐ Gudavalli MR: Estimation of dimensional changes in the lumbar intervertebral foramen of lumbar spine during flexion distraction procedure. Proceedings of the 1994 International Conference on Spinal Manipulation, June 10‐11, 1994, Palm Springs, CA, pp 81.
3 ‐ Gudavalli MR, Cox JM, Baker JA, Cramer GD, Patwardhan AG: Intervertebral Disc Pressure Changes During a Chiropractic Procedure. Proceedings of Bioengineering Conference, Phoenix, 1997
4 ‐ Gudavalli MR, Cox JM, Baker JA, Cramer GD, Patwardhan AG: Intervertebral Disc Pressure Changes
During The Flexion‐Distraction Procedure for Low Back Pain, Proceedings of the International Society for the Study of the Lumbar Spine, Singapore 1997