

Case Report
Treatment and Outcomes of a 30-year-old Female Managed with Cox® Flexion-Distraction Therapy for Right C4/5 Posterolateral and C5/6 Posterocentral Disc Protrusions.
AUTHOR: Dr Danica Newbold (B.HSci (Chiro), M.Clin.Chiro, Ad.Dip Myo) Malvern Chiropractic and Melbourne Spine Clinic (Melbourne, Australia).
History:
Mrs J is a 30-year-old customer service representative who presented to Malvern Chiropractic and Melbourne Spine Clinic on 28 December 2017. She described severe right-sided cervical pain and radicular symptoms, extending into the right arm and hand. The pain was described as a “sharp, shooting” pain that restricted all movements of the head and neck. Mrs J was also unable to lift her arm above 20 degrees (approximate) and grip anything in her right hand. Initial VAS scores were noted at 8-8.5/10. The pain was aggravated by movement, lying in bed, and sitting at her workplace. Due to her pain levels, Mrs J was not working currently and unable to complete regular activities of daily living (ADLs).
Mrs J’s symptoms had begun four (4) months before presentation after she and her husband had moved house. Symptoms were insidious and progressive over a one (1) month period and steadily worsened. She visited her local general practitioner (GP) in October 2017, who prescribed Lyrica, Panadine Forte, and Tramadol for her pain and advised to seek treatment from a Physiotherapist. She attended two (2) sessions with a Physiotherapist; however, her pain levels increased. She immediately ceased treatment and researched alternative methods for relief of her current pain and symptoms. Mrs J’s was also referred for imaging (by her general practitioner) of the cervical spine, and an MRI was performed on 19 October 2017.
Examination findings:
An initial examination performed on 28 December 2017 revealed the following:
Range of Motion (ROM):
Severely reduced active and passive flexion and lateral flexion of the cervical spine with moderately reduced rotation (L>R). Pain was reproduced on all movements.
Palpation:
Hypertonic and tender long cervical spinal musculature extending into the trapezius, rhomboids, infraspinatus, and teres group (major and minor) of the right. Spinal joint tenderness and rigidity were noted over C4-C6 levels on the right side.
Neurological and Orthopaedics:
Reflexes were tested and noted as:
Absent at C5 (Biceps) and C6 (Brachioradialis) on the right
Reduced (+1) at C7 (Triceps) on the right.
Myotomal screening revealed weakness at all right-sided muscles due to pain reproduction. The following values were noted at the initial examination:
Supraspinatus right 2/5,
Biceps right 2/5,
Wrist extensors right 4/5,
Deltoid right 2/5,
Triceps right 4/5,
Wrist flexors right 4/5.
Reduced (+1) at C7 (Triceps) on the right.
Orthopedic testing returned positive results for cervical compression and maximal cervical compression tests on the right (negative reproduction of radiculopathy).
Imaging:
MRI scans conducted on 19 October 2017 reported:
“desiccation of the C4/5 disc associated with a posterolateral disc protrusion on the right. This contacts the right C5 nerve root at the entrance to the neural foramen. More centrally, there is contact with the right anterior surface of the cord (without cord compression or abnormal cord signal)”.
This same report also mentioned at C5/6:
“mild disc desiccation and shallow posterocentral disc protrusion. This lies just shy of the anterior surface of the cord. Cord morphology and signal is within normal limits, and there was no foraminal narrowing at this level”.
The 2017 images have been misplaced and cannot be included in this study. The 2019 images were ordered at the request of the patient given the outcomes of her treatment plan.
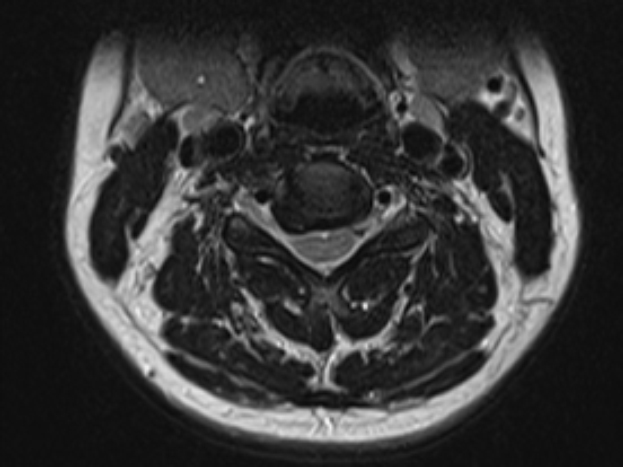
Repeat MRI scans performed on 25 November 2019 revealed:
“At C4/5, a large right posterolateral disc osteophytic protrusion. This contacts the exiting right C5 nerve rootlet. No neural foraminal stenosis”.
“Minimal disc osteophytic bulge at C5/6 with mild central canal narrowing. No neural foraminal stenosis”.
Please refer to corresponding images below (Fig 1 and 2).

Treatment and results:
Mrs J was treated using Cox® Flexion-Distraction and Spinal Decompression Therapy over several sessions focusing on the right C4/5 discal compartment decompressing the C5 nerve root irritation and C5/6 posterocentral discal derangement.
At session one (1) the patient was relatively hypersensitive. Following on from tolerance testing prior to therapy application the patient could only manage to receive long y-axis distraction (‘5-4-3 Method” – 5 repetitions, over 4 seconds in 3 groups) and soft tissue to the cervical and right shoulder musculature. The patient was advised to conduct self-care at home post-treatment consisting of rest and cryotherapy (cold/ ice packs)- 10 minutes of cold/ice pack use every hour for 24 hours.
At session two (2), on 30 December 2017, with no increase in pain levels post-treatment, flexion-distraction protocol I (1) was performed on the cervical spine (long y-axis traction and flexion only). Treatment included targeted soft tissue therapies, including trigger point release of the right levator scapulae and rhomboid muscles.
By session three (3) on 2 January 2018, Mrs J was able to abduct her arm further (approximately 30-40 degrees), and her pain levels had decreased slightly (VAS = 7/10). Flexion-Distraction protocol II (2) (long y-axis traction, flexion, lateral flexion and coupling movements by 20 repetitions) was implemented at this session (at approximately 50 % intensity) and continued throughout the treatment plan, increasing the movements within the patients’ tolerance with each subsequent session.
By session five (5) on 6 January 2018, Mrs J reported that her pain levels had decreased to a VAS score 4/10 (50% improvement), her arm pain was no longer restricting any movements of the shoulder or grip strength in the right hand. She was able to abduct the arm/shoulder above 90 degrees. At this time, Mrs J was prescribed stretches for the cervical spine and right shoulder to support her overall recovery.
During this initial stages of her treatment program, Mrs J felt that reduced work hours would aid in her recovery. She indicated that she had noticed after long hours at work a fatigue type feeling towards the end of the day, which subsequently increase her neck and arm pain. A six-eight-week period of 50% reduced work hours was conducted and allowed the patient to rest and recover effectively. During this time, Mrs J was able to also focus on her prescribed rehabilitation program.
Prognosis:
Mrs J progress through the treatment program was excellent and was able to return to regular ADL’s quite quickly. She attended her sessions as indicated and, by appointment number 13 (12 weeks post initial consultation) was able to shift to a maintenance style program (monthly sessions).
Re-evaluation of the initial examination findings demonstrated an overall improvement in ROM to full and pain-free movements. Orthopaedic and neurological testing indicated inconsequential compromise at the C4/5 and C5/6 levels.
Due to the nature of her occupation (call centre customer service), discussions about posture and ergonomics had been included as part of the overall treatment plan. Modifications to the patients working environment, including using standing desks where possible, taking regular breaks to readjust posture and perform exercises/ stretches, and having a desk/ workstation assessment conducted with an Occupational Therapist were implemented.
Mrs J continues to attend regular appointments in our clinic and maintains a 90-100% improvement in pain and discomfort levels overall. She continues to receive Cox® Flexion-Distraction Protocol II (2), targeted soft tissue therapies and low force Activator-style adjustments to the thoracic spine.
Conclusion:
Cox® Flexion-Distraction and Spinal Decompression Therapy was the appropriate method of treatment for this patient’s condition, as demonstrated by the successful subjective and objective outcomes achieved.
While the patient currently does not display any of her original signs and symptoms, she continues to receive monthly treatment to maintain her pain-free lifestyle. Occasionally, Mrs J indicates mild stiffness and tightness of the cervicothoracic region, but overall, she is very pleased with the outcomes achieved thus far and can continue her regular ADL’s.
References: Cox JM, Feller J, Cox J. Distraction Chiropractic Adjusting: Clinical Application and Outcomes of 1000 cases. (1996).
Hassan F, Osama M, Ghafoor A. Effects of Oscillatory Mobilization as Compared to Sustained Stretch Mobilization in the Management of Cervical Radiculopathy: A Randomised Controlled Trial. (2019).
Low Back Pain: Mechanisms, Diagnosis and Treatment. James M Cox. 7th Ed. Lippincott, Williams & Wilkins. 2011.
| Monday – Friday | 8am – 6pm |
| Saturday | 8am - 11am |
After hours contact by appointment only on (03) 9822 1835
